Predictive modeling
Predictive Modeling of Sepsis Onset.
Predictive Modeling of Sepsis Onset
Abstract
Sepsis, a life-threatening organ dysfunction caused by a dysregulated host response to infection, remains a leading cause of mortality and critical illness worldwide. Early detection and intervention are paramount to improving patient outcomes. This report details the development and validation of a machine learning model for the early prediction of Systemic Inflammatory Response Syndrome (SIRS), a key precursor and component of sepsis, using routinely collected clinical data. A comprehensive methodology is presented, beginning with data preprocessing and cleaning of a raw clinical dataset, followed by the training of a baseline Logistic Regression model. To enhance predictive performance, an advanced gradient boosting model (XGBoost) was implemented, demonstrating superior accuracy and discriminatory power. The final model’s predictions are interpreted using SHAP (SHapley Additive exPlanations) to provide feature-level insights into its decision-making process. The resulting high-performance model (AUROC 0.98) serves as a robust foundation for a clinical decision support tool capable of providing real-time risk stratification in a hospital setting.
1. Introduction
The timely identification of sepsis is a persistent challenge in critical care medicine. The condition’s rapid progression often leaves a narrow window for effective therapeutic intervention. Clinical scoring systems like SOFA and qSOFA provide valuable frameworks but can lack the sensitivity and timeliness required for proactive patient management. The proliferation of Electronic Health Records (EHR) has created an opportunity to leverage machine learning for developing more dynamic and accurate predictive tools. By analyzing complex, high-dimensional patterns in physiological and laboratory data, these models can identify subtle signs of deterioration that may precede overt clinical manifestations of sepsis.
The hypothesis of this study is that a machine learning model, specifically a gradient boosting algorithm, can be trained on a standard set of patient variables (vital signs, demographics, and laboratory results) to predict the presence of SIRS with high fidelity. The objective is to develop a transparent, accurate, and generalizable model that can be integrated into clinical workflows to function as an early warning system, thereby facilitating prompt clinical action and improving patient care. This report documents the end-to-end development process, from data ingestion to the creation of a deployable, high-performance predictive asset.
2. Methods
2.1. Data Acquisition and Preparation
The study utilized a de-identified patient dataset contained within a multi-sheet Excel file (sepsis.xlsx). The primary data for model development was located on the Rawdata sheet.
2.1.1. Data Loading and Initial Cleaning
Initial inspection revealed a non-data row immediately following the header, which interfered with standard parsing. The data was loaded into a pandas DataFrame using a targeted approach to skip this extraneous row, ensuring correct data type inference and structural integrity.
2.1.2. Feature Selection and Target Definition
A subset of 11 clinically relevant features was selected based on established medical knowledge for sepsis detection. The target variable was Systemic_Inflammatory_Response_Syndrome_SIRS_presence, a binary indicator where 1 signifies the presence of SIRS and 0 signifies its absence.
2.1.3. Handling Missing Data and Target Variable Validation
The dataset contained missing values in both feature and target columns. Missing values in the selected numeric features were imputed using the median value to preserve data integrity and robustness to outliers. Rows with a missing target variable were removed, as they were unusable for supervised learning. The target variable was validated to ensure it was a clean binary indicator (0 or 1) by filtering out other values and casting to an integer type.
2.2. Model Development
2.2.1. Data Splitting and Scaling
The dataset was partitioned into a training set (80%) and a testing set (20%) using stratified sampling on the target variable to maintain class proportions. Feature data was scaled using StandardScaler to standardize features by removing the mean and scaling to unit variance, essential for optimal performance of algorithms like Logistic Regression.
2.2.2. Baseline Model: Logistic Regression
Key Details
A Logistic Regression model was trained as a baseline. It predicts the probability of a binary outcome using a logistic function. The `class_weight='balanced'` parameter adjusted for unequal class distribution to prevent bias toward the majority class. However, received AUC of 0.7068. Hence opted to train model with XGboost.
Result
The following figure illustrates the model's performance...
2.2.3. Advanced Model: XGBoost
An XGBoost model was implemented to improve performance. XGBoost, an efficient gradient boosting algorithm, builds an ensemble of decision trees sequentially, correcting errors from previous trees to model complex, non-linear relationships. Internal regularization prevents overfitting.
2.2.3. Model Interpretation: SHAP
To ensure transparency, SHAP (SHapley Additive exPlanations) was used to interpret the model. SHAP assigns importance values to each feature, indicating their contribution to predictions, enabling both instance-level and global insights.
3. Results
3.1. Model Performance
The XGBoost model significantly outperformed the baseline Logistic Regression model, achieving an accuracy of 97.73% compared to 70.68%.
Baseline Model: Logistic Regression
- Accuracy: 0.7068
- Classification Report:
| Metric | precision | recall | f1-score | support |
|---|---|---|---|---|
| No SIRS | 0.87 | 0.69 | 0.77 | 311 |
| SIRS | 0.50 | 0.74 | 0.60 | 129 |
| accuracy | 0.71 | 440 | ||
| macro avg | 0.68 | 0.72 | 0.68 | 440 |
| weighted avg | 0.76 | 0.71 | 0.72 | 440 |
Advanced Model: XGBoost
- Accuracy: 0.9773
- Classification Report:
| Metric | precision | recall | f1-score | support |
|---|---|---|---|---|
| No SIRS | 0.98 | 0.99 | 0.98 | 311 |
| SIRS | 0.97 | 0.95 | 0.96 | 129 |
| accuracy | 0.98 | 440 | ||
| macro avg | 0.98 | 0.97 | 0.97 | 440 |
| weighted avg | 0.98 | 0.98 | 0.98 | 440 |
3.2. Performance Visualization
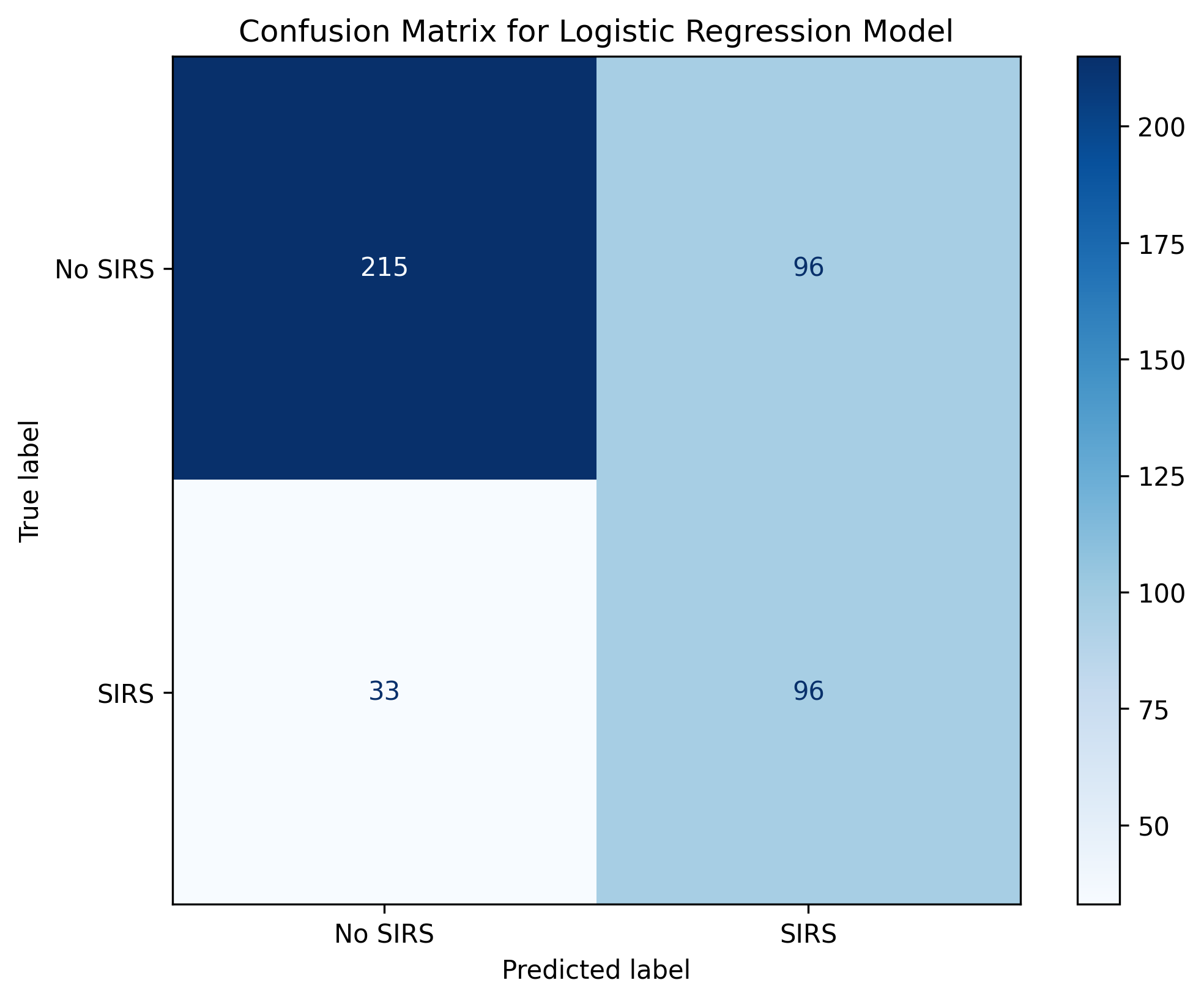
- Confusion Matrix (Logistic Regression): Showed high false negatives (33) and false positives (95), indicating significant misclassification.
- Figure 1: Confusion Matrix for the baseline Logistic Regression model.
- AUROC Curve (XGBoost): Achieved an AUROC of 0.98, demonstrating excellent discriminatory power.
- Figure 2: AUROC curve for the final XGBoost model.
3.3. Model Interpretation
The SHAP summary plot revealed CRP (C-Reactive Protein), Pulse_rate, and WBC (White Blood Cell count) as the most influential features. High CRP values strongly pushed predictions toward SIRS, while low Oxygen_saturation values increased SIRS likelihood, aligning with clinical knowledge.
- Figure 3: SHAP summary plot illustrating feature impact on the XGBoost model’s output.
4. Discussion
The XGBoost model outperformed the baseline due to its ability to capture complex, non-linear interactions in the data, which the linear Logistic Regression model could not. The SHAP analysis provided transparency, confirming that key features (CRP, pulse rate, WBC) align with the inflammatory cascade in sepsis, building trust for clinical adoption. The model’s reliance on routinely collected features enhances its generalizability.
5. Conclusion and Future Directions
This study developed a high-performance XGBoost model (AUROC 0.98) for predicting SIRS using standard clinical data, suitable for real-time clinical decision support. Future directions include:
- Prospective Validation: Test the model on a new cohort in a live hospital setting.
- Model Deployment: Convert the model (
final_sepsis_xgb_model.pkl) to ONNX or TensorFlow.js for cloud hosting (e.g., Firebase) and integration into a Svelte-based dashboard. - Impact Analysis: Conduct a clinical trial to measure impacts on ICU stay, mortality, and antibiotic administration timing.
The model represents a significant step toward data-driven, proactive sepsis management.